- Research
- Open access
- Published:
Speckle tracking of left ventricle in pediatric patients with hemodynamically significant patent ductus arteriosus (PDA): case–control study
Egyptian Pediatric Association Gazette volume 72, Article number: 86 (2024)
Abstract
Background
Left ventricle (LV) volume overload is observed with hemodynamically significant PDA as it causes left to right shunting, leading to increased pulmonary blood flow. This overload causes LV remodeling as LV increases stroke volume in trial for compensation, but in larger shunts, patients may develop symptoms of congestive heart failure. Two-dimensional (2D) speckle-tracking echocardiography has emerged as a technique for objective and quantitative evaluation of global and regional myocardial function, independent of the angle of myocardial insonation.
Aim of the work
This study aimed to evaluate left ventricular function by 2-dimensional speckle tracking in children with hemodynamically significant PDA.
Methods
This prospective controlled study was performed on 54 children divided into two groups (34 as cases and 20 as controls) to compare echocardiographic measurements. Conventional Echocardiography, tissue Doppler, and Speckle tracking were done for all patients, and measurements were compared.
Results
There was a statistically significant difference (p value < 0.001) in global longitudinal strain (GLS) in the PDA group indicating a decrease in LV function in PDA patients. This difference was observed in several conventional echocardiographic parameters but not in tissue Doppler in our study.
Conclusion
Left ventricle global strain is an important predictor of the myocardial performance index of the Left ventricle in patients with hemodynamically significant PDA and outweighs other conventional echocardiographic parameters and tissue Doppler indices.
Background
Left ventricle (LV) volume overload is observed with hemodynamically significant PDA as it results in the shunting of blood from the left ventricle to the right ventricle increasing pulmonary blood flow. This overload causes LV remodeling as LV increases stroke volume in trial for compensation, but in larger shunts, patients may develop symptoms of congestive heart failure [1].
The hemodynamic effects of PDA differ between different patients. The pulmonary vascular resistance drops significantly at birth, so a continuous left-to-right shunt develops if an infant suffers from PDA. According to the Poiseuille Law, this shunt has a positive relationship to the pressure gradient between the aorta and pulmonary artery and a negative relationship to the resistance to flow. The pulmonary and systemic resistances change significantly in patients with large PDA while this is not observed in smaller ones due to high resistance. There are adjustable factors that affect pulmonary vascular resistance like oxygen tension and blood PH which affect trans-ducal flow [2].
A left‐to‐right shunt from PDA results in increased pulmonary blood flow. The level of this shunt and its connected cardiopulmonary effect determines the pathophysiologic characteristics of this lesion in clinical care. Special hemodynamic characteristics associated with premature neonates make them more vulnerable to PDA‐associated cardiorespiratory compromise. PDA left to right flow causes increased pulmonary blood flow and dilatation of the left heart. This results in increased left ventricular end‐diastolic pressures, which elevates pulmonary venous pressure, and pulmonary congestion. This effect is well observed in preterm neonates because of the greater adaptability of their immature ventricles [3].
Two-dimensional (2D) speckle tracking is a new echocardiography technique developed for functional and quantitative assessment of myocardium globally and regionally regardless of myocardial insonation angle [4].
The main advantage of this new technique is not just it assesses the global myocardial function, but also that it detects any changes in regional myocardial deformation changes that cannot be visualized using the usual 2D parameters [5].
Aim of work
The aim of this study was to evaluate left ventricular function by 2-dimensional speckle tracking in children with hemodynamically significant PDA.
Methods
This study is a prospective analytical case–control study on 34 infants and children. This study was conducted at a tertiary care university hospital from November 2022 to January 2024, with audible PDA.
A control group consisting of 20 healthy infants and children was included in the study for comparison of echocardiographic measurements.
Inclusion criteria
Patients in pediatric age ranging from 6 months to 18 years whose weight is over 6 kg with audible PDA with or without evidence of LV volume overload were included in the study.
Exclusion criteria
-
Patients with PDA not eligible for transcatheter closure
-
Patients with PDA suffer from other significant congenital heart diseases or irreversible pulmonary vascular diseases.
Patients evaluation
All Participants were evaluated as follows: complete history taking, full examination with special emphasis on anthropometric measurements, and local examination with detailed cardiac examination.
Investigations
All children were submitted to routine investigations, chest X-ray, ECG, and detailed transthoracic echocardiography (TTE) using different modes including 2D TTE, tissue Doppler imaging (TDI), and 2D STE.
-
A-Routine echocardiographic examination
-
B- Examination using tissue Doppler.
-
C- Speckling tracking imaging 2D echocardiography
Equipment
-
Machine: echocardiographic evaluation was done using a commercially available ultrasound transducer and equipment (Vivid E95, GE Healthcare, Horten, Norway).
-
Transducers: data acquisition was performed with a 3.5-MHz transducer, S7 probe. Workstation: Digital loops were obtained and analyzed using AFI software on the Equipment.
A) Routine echocardiographic examination
The study was done for all participants (cases and controls) using the standard views (apical, parasternal long axis, parasternal short axis, and subcostal) to gather all data required for comparison according to the American Society of Echocardiography guidelines (Figs. 1, 2, 3, and 4) [6].

Apical 4 chamber view of 7-month-old patient with PDA

M mode from PLAX view of 7-month-old patient

Modified parasternal short axis view showing Hemodynamically significant PDA in 1-year-old patient measuring 3 mm at the pulmonary end

PW-Doppler in PDA patient showing EA ratio 1.53
B) Examination using tissue Doppler (TDE)
-
Mitral annulus velocities:
PW-TDI sample volume is positioned at the septal mitral annulus producing three waves, an antegrade systolic wave S', and two retrograde waves, E' representing passive LV filling and A' wave representing atrial contraction.
-
Myocardial performance index of left ventricle (MPI):
The MPI was calculated using the Tei index which equals the difference between a’ and b’ divided by b’. a’ is the time from the end of the A'-wave to the beginning of the E'-wave and b’ is the time duration of the S' wave (Fig. 5).
Fig. 5 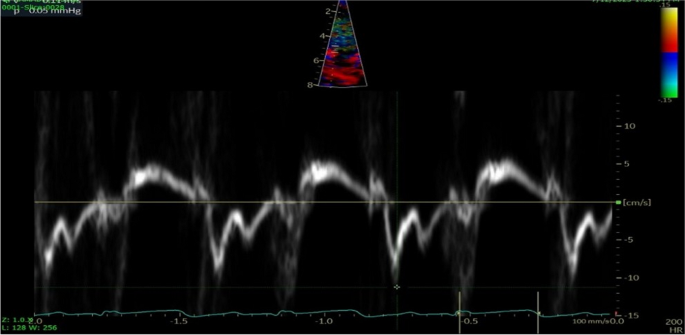
Tissue Doppler of 1.5-year-old patient with PDA, TEI index 0.62

C) Speckling tracking imaging transthoracic 2D echocardiographic examination
A 3.5-MHz transducer, S7 probe interfaced with a GE Vivid E95 ultrasound system was used to image each heart. We used the 2D LVQ AFI function of the device to assess global longitudinal, circumferential, and radial strain and area strain. Three views were obtained 4 chambers, 2 chambers, and APLAX (Figs. 6, 7, and 8 respectively).

4-chamber view for AFI LV strain calculation

2-chamber view for AFI LV strain calculation

3-chamber view for AFI LV strain calculation
The speckle tracking of the left ventricle was done beginning from a region of interest (ROI) defined at the end of the systole. 2D strain analysis was performed at the end of the process in the 2D auto left ventricular auto quantification tool, which also calculated the volume and mass of the left ventricle. The meshes obtained from the two measurements were used for the 2D ROI strain. The 2D ROI strain was generated in an automatic manner using the end-systolic frame and was generated from an endocardial and an epicardial mesh (Fig. 9). The mesh of the endocardium was dependent on the one used for the measurement of end-systolic volume (ESV). The mesh of epicardium was produced automatically from the epicardial mesh used in the stage of left ventricle mass, by generating it from the end of diastole to the end of systole. The operator can adjust the shape of ROI by putting drawer points to pull the nearby ROI border towards where the operator wants it to go from the results of tracking, several parameters result from 2D strain, including longitudinal, circumferential, area, and radial strain.

Bull’s eye of a 1.5-year-old patient with hemodynamically significant PDA. GS was 18.4%
Assessment of variability
For the assessment of intra-observer variability, the same operator twice measured the analysis of the 2D strain of 15 participants who were selected randomly at an interval of 2 months to avoid recall bias. For interobserver variability assessment, the measurements of 2D strain were operated by a second observer who was not informed of the results of the first operator.
Statistical analysis and data interpretation
SPSS software, version 25 (SPSS Inc., PASW statistics for Windows version 25. Chicago: SPSS Inc.) was used for the analysis of data. Number and percent described qualitative data. Median (minimum and maximum) used in quantitative data for non-normally distributed data and mean (Standard deviation) for normally distributed data after using the Kolmogrov-Smirnov test or testing normality.
The judgment of the result’s significance was at the (≤ 0.05) level.
-
We used chi-square, Monte Carlo tests, and Fisher exact test for qualitative data comparison between groups.
-
We used the Mann–Whitney U test for comparison between 2 studied groups for non-normally distributed data.
-
We used the Student t-test for comparison of the 2 independent groups for normally distributed data.
-
We used the Wilcoxon signed rank test for comparison between 2 studied periods for non-normally distributed data.
Results
Regarding demographic data, there was a statistical difference regarding weight and BSA in the PDA group with a p value < 0.001* as illustrated in Table 1.
Regarding clinical presentation of PDA cases, the most common complaint was repeated chest infection in 27 cases (80%). Four cases were asymptomatic and discovered incidentally by PDA murmur auscultation in routine clinical examination as illustrated in Fig. 10.

Funnel chart of clinical presentation of PDA cases
LVIDD in PDA cases was statistically significantly higher than in the control group, with z score p value less than 0.001 as illustrated in Table 2 and Fig. 11.

Box and whisker plot of LVIDd and z score in PDA cases and control
Some of the conventional echocardiographic M mode indices were significant and indicated dilated left ventricle-like interventricular septum thickness in diastole (IVSd) and in systole (IVSs), the posterior wall thickness in systole of the left ventricle (LVPWs) and Stroke volume (SV) as indicated in Table 3 and Fig. 12. LA/AO ratio is statistically significant between 2 groups indicating LA dilation in PDA cases.

Box and whisker plot of M mode findings in PDA cases and control
Pulsed wave Doppler showed increased E and A velocity across the mitral annulus while the E /A ratio was not statistically different as illustrated in Table 4.
Tissue Doppler findings in PDA cases show statistically significant increased A velocity while the Tei index was increased but not statistically significant as illustrated in Table 5.
Speckle tracking comparison showed that all global strain in all acquired views was statistically lower in the PDA group with p value < 0.05 except peak strain dispersion (PSD) which was lower but not statistically significant as illustrated in Table 6 and Figs. 13, 14 and 15.

Box and whisker plot of PW Doppler

Box and whisker plot of tissue Doppler

Box and whisker plot of speckle tracking of LV
Discussion
Our study was performed to evaluate left ventricle function with 2-dimensional speckle tracking echocardiography and to evaluate if there is an advantage of speckle tracking over conventional echocardiography techniques and tissue Doppler in detecting changes in left ventricle systolic function.
Clinical data showed that the most presenting clinical manifestation to hospital or outpatient clinics in this PDA group was repeated chest infections (80%), poor weight gain (75%), dyspnea (60%), and difficulty in feeding (50%). This observation agrees with the clinical Scenario of PDA children who commonly suffer from failure to thrive, difficulty in feeding, and dyspnea depending on the size of the PDA and quantity of left-to-right shunting [7].
In our study, the PDA patient’s median age was 2 years (ranging from 6 months to 14 years), This was matched with controls of close age to not affect the measured echocardiographic indices.
Demographic data revealed that the median weight of the PDA group was 10 kg (ranging from 6 to 43 kg), BSA median was 0.49 (ranging from 0.31 to 1.39). These parameters were statistically significantly lower than the control group which illustrates the effect of PDA on the growth parameters of children, especially weight. This was reported in a study by Kunel et al. which studied premature infant that was managed by PDA surgical closure and observed flattering of their growth [8].
Conventional echocardiography M mode parameters illustrated that LVIDd was increased in the PDA group and by calculation of the z score, it was higher than the control group. Both parameters were statistically significantly higher. This is because of volume overload that occurs in hemodynamically significant PDA [9].
Also with conventional echocardiography M mode, IVSd, IVSs, and LVPWs were increased with statistical differences in the control group which indicates hypertrophy of the left ventricle due to volume overload of the heart. Also stroke volume was increased in the PDA group due to dilatation and hypertrophy of the Left ventricle according to Frank Sterling Law [10].
Regarding PW Doppler echocardiography A velocity and E velocity were statistically significantly higher in the PDA group in relation to the control group while the E/A ratio was lower than that of the control but was not statistically significant. This increase in E velocity is mainly due to an increase in LA pressure due to diastolic dysfunction [11]. E/A ratio is within normal level due to increased E velocity as well as increased A velocity this represents grade 2 diastolic dysfunction [12].
Regarding the tissue Doppler, the Tei index was increased in the PDA group but not statistically different from the control. The Tei index evaluates the performance of the myocardium (MPI) and is used to detect combined ventricular systolic and diastolic function [13]. The MPI value has an inverse relationship to myocardial function; if MPI is increased, this indicates global myocardial function deterioration [14]. In a study by Zhou et al., the Tei index of children diagnosed with PDA was statistically significantly higher than that of the control group (p < 0.05) [15]. The Tei index was higher but not statistically significant in our study. A/ velocity was statistically significantly increased due to increased atrial filling pressure during atrial contraction in late diastole because of impaired diastolic function of the left ventricle. The pressure of the left atrium is elevating with the reduction in left ventricular compliance [16].
Regarding speckle tracking of LV, all values of global strain in the 4-chamber and 2-chamber view and APLAX view were statistically significantly lower than comparing controls with p value < 0.001. we used the LV AFI method for the calculation of global strain after good acquisition of images in the views with automated results of Global strain and Bull’s eye of LV strain which was also statistically significantly lower than comparing controls with p value < 0.001. The median average GS was − 19.9 (ranging from − 16 to − 23). Although these results are within normal values of LV strain, in comparison with controls, it indicates impaired systolic function of LV in the PDA group. This is compatible with other studies published in the literature which indicated that global longitudinal strain (GLS) of the left ventricle is a useful single predictor of MPI in PDA patients before and after PDA surgical or percutaneous closure [17].
Global longitudinal strain in our study and other studies is impaired in PDA patients indicating the effect of PDA on the left ventricle myocardial performance index. Unlike other echocardiography parameters like LVIDd which was elevated in our study but in other studies was not different from control [18]. While the E/A ratio was not impaired in our study, it was impaired in other studies [15]. Also, the tissue Doppler Tei index was not statistically different from controls in our study while in other studies it was statistically elevated in PDA patients like the study by Agha et al. [17]. This means that GLS could be the useful sole indicator of LV function in patients with hemodynamically significant PDA.
Limitations
The number of PDA cases and healthy controls were relatively small. Another limitation was that our study didn’t include neonates suffering from PDA, this was because of the study settings as we included the PDA cases who were planned for percutaneous PDA closure from the catheterization clinic in our hospital. Also, while performing 2DSTE there was difficulty in adjusting speckles on the region of interest by the current available software. So, Software packages need to be adjusted to be suitable for children less than 20 kg.
Conclusion
Left ventricle global strain is an important predictor of the myocardial performance index of the left ventricle in patients with hemodynamically significant PDA and outweighs other conventional echocardiographic parameters and tissue Doppler indices.
Availability of data and materials
All data generated or analyzed during this study are included in this published article and its supplementary information files could be obtained after communication with the corresponding author.
References
Gupta SK, Krishnamoorthy KM, Tharakan JA, Sivasankaran S, Sanjay G, Bijulal S, Anees T (2011) Percutaneous closure of patent ductus arteriosus in children: Immediate and short-term changes in left ventricular systolic and diastolic function. Ann Pediatr Cardiol 4(2):139–144
Hundscheid T, van den Broek M, van der Lee R, de Boode WP (2019) Understanding the pathobiology in patent ductus arteriosus in prematurity—beyond prostaglandins and oxygen. Pediatr Res 86(1):28–38
Backes CH, Hill KD, Shelton EL, Slaughter JL, Lewis TR, Weisz DE, Mah ML, Bhombal S, Smith CV, McNamara PJ (2022) Patent ductus arteriosus: a contemporary perspective for the pediatric and adult cardiac care provider. J Am Heart Assoc 11(17):e025784
Adda J, Mielot C, Giorgi R, Cransac F, Zirphile X, Donal E, Sportouch-Dukhan C, Réant P, Laffitte S, Cade S (2012) Low-flow, low-gradient severe aortic stenosis despite normal ejection fraction is associated with severe left ventricular dysfunction as assessed by speckle-tracking echocardiography: a multicenter study. Circ Cardiovasc Imaging 5(1):27–35
Alharthi MS, Jiamsripong P, Calleja A et al (2009) Selective echocardiographic analysis of epicardial and endocardial left ventricular rotational mechanics in an animal model of pericardial adhesions. Eur J Echocardiogr 10:357–362
Lang RM, Bierig M, Devereux RB et al (2005) Recommendations for chamber quantification: a report from the American Society of Echocardiography’s Guidelines and Standards Committee and the Chamber Quantification Writing Group, developed in conjunction with the European Association of Echocardiography, a branch of the European Society of Cardiology. J Am Soc Echocardiogr 18(12):1440–1463
Schneider DJ, Moore JW (2006) Patent ductus arteriosus. Circulation 114(17):1873–1882
Babla K, Dassios T, Pushparajah K, Hickey A, Greenough A (2021) Premature infants with patent ductus arteriosus: postnatal growth according to type of management. Pediatr Neonatol 62(1):36–40
Fadel, Bahaa & Mohty, Dania & Husain, Aysha & Dahdouh, Ziad & Al Admawi, Mohammed & Pergola, Valeria & Di salvo, Giovanni. (2015). The various hemodynamic profiles of the patent ductus arteriosus in adults. Echocardiography (Mount Kisco, N.Y.) 32. https://doi.org/10.1111/echo.12943
de Freitas Martins F, Ibarra Rios D, Resende MH, Javed H, Weisz D, Jain A, de Andrade Lopes JM, McNamara PJ (2018) Relationship of patent ductus arteriosus size to echocardiographic markers of shunt volume. J Pediatr 202:50-55.e3. https://doi.org/10.1016/j.jpeds.2018.06.045
Nagueh SF, Smiseth OA, Appleton CP, Byrd BF 3rd, Dokainish H, Edvardsen T, Flachskampf FA, Gillebert TC, Klein AL, Lancellotti P, Marino P, Oh JK, Popescu BA, Waggoner AD (2016) Recommendations for the evaluation of left ventricular diastolic function by echocardiography: an update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J Am Soc Echocardiogr 29(4):277–314
Mitter SS, Shah SJ, Thomas JD (2017) A test in context: E/A and E/e′ to assess diastolic dysfunction and LV filling pressure. J Am Coll Cardiol 69(11):1451–1464
Al-Fahham MM, Mahmoud EM, Abdel Gawad T (2022) Assessment of left and right ventricular Tei indices in critically ill children with septic shock. Prog Pediatr Cardiol 65:101491
Bokiniec R, Własienko P, Borszewska-Kornacka MK et al (2016) Myocardial performance index (Tei index) in term and preterm neonates during the neonatal period. Kardiol Pol 74:1002–1009. https://doi.org/10.5603/KP.a2016.0056
Zhou X-L, Huang D-B, Zhu Q (2010) Tei index in assessment of cardiac function in children with congenital heart diseases before and after transcatheter closure. Chin J Med Imag Technol 26:1447–1449
Yalçin F, Kaftan A, Muderrisoğlu H, Korkmaz ME, Flachskampf F, Garcia M, Thomas JD (2002) Is Doppler tissue velocity during early left ventricular filling preload independent? Heart (British Cardiac Society) 87(4):336–339
Agha HM, Hamza HS, Kotby A, Ganzoury MEL, Soliman N (2017) Predictors of transient left ventricular dysfunction following transcatheter patent ductus arteriosus closure in pediatric age. J Saudi Heart Assoc 29(4):244–251
Amoogzar H, Shakiba AM, Derakhshan D, Ajami G, Cheriki S, Borzouee M, Edraki MR, Mehdizadegan N (2015) Evaluation of left ventricular function by tissue Doppler and speckle-derived strain rate echocardiography after percutaneous ductus closure. Pediatr Cardiol 36:219–225
Acknowledgements
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Author information
Authors and Affiliations
Contributions
AB performed the clinical examination, did echocardiography, contributed to data interpretation, and drafted the work. OA shared in data interpretation and revised discussion. ME performed the statistical analysis and contributed to the interpretation of the results and writing the discussion. HA formatted the study design, rechecked the echocardiography of the sample of cases and control, and contributed to data interpretation and discussion revision. All authors have participated in drafting the manuscript. All authors read and approved the final version of the manuscript. All authors contributed equally to the manuscript and read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study followed the Principles of the Declaration of Helsinki and was approved by the Ethical Review Committee of Kafrelsheikh University registered with approval code (MKSU 50–8-1) and informed written parental consent from all participants in the research.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Baz, A.M.K., El-Agamy, O.A.EF., Eldegwi, M. et al. Speckle tracking of left ventricle in pediatric patients with hemodynamically significant patent ductus arteriosus (PDA): case–control study. Egypt Pediatric Association Gaz 72, 86 (2024). https://doi.org/10.1186/s43054-024-00326-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s43054-024-00326-7